
By Amy Uccello, Sr. AYSRH Technical Advisor, PSI
Adolescents 360 (A360) always dared to be bold.
We launched at the 2016 International Conference on Family Planning (ICFP) with an ambitious hypothesis: by fusing a transdisciplinary approach with a Human-Centered Design (HCD) process, we could unleash breakthrough solutions to increase adolescent girls’ access to modern contraception in Nigeria, Tanzania and Ethiopia — and beyond.
Would it work?
Over the past three decades, projects across our field have contributed to the evidence-base of best practices for adolescent girls to uptake modern contraception. But despite major investments, scale-able interventions remain elusive.
Seven in 10 girls aged 15-19 across Sub-Saharan Africa still want but don’t have access to contraception. Half of pregnancies among this cohort are unintended, and one in two will end in abortion—the majority of which are unsafe, placing girls in dire risk of adverse health outcomes. The cost of sticking to the status quo outweighed the risk of trying.
So we took the leap.
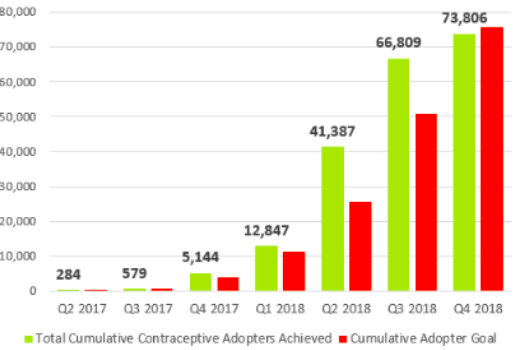
In the two years since announcing A360 – and the 11 months since launching prototypes – we, in partnership with more than 280 young people, have unveiled four interventions across three countries cost-effectively and at high speed. We’ve sourced from deep consumer insights to change the conversation around contraception, and we’ve done it by overlaying the process with a motley crew of disciplines who forged and refined A360’s solutions. Since January 2018, we’ve inspired and served more than 73,000 girls with contraception (figure 1). One in two girls who engages with A360 voluntarily takes up a method, half of which are long-acting reversible contraceptives.
Figure 1: Cumulative Voluntary Adopters as of September 2018
(Actual v. Adopter Goal)

This ICFP, A360 will spotlight the inroads we have made: a blueprint for how to work with and for young people to spark girl-defined AYSRH solutions; an evidence-based adaptive implementation roadmap to guide public health practitioners through the journey to scale; a technical case study of A360’s experience in Tanzania; and the myriad of learnings demonstrating that when evidence-based best practices are combined – and combined with a team that offers a wide-range of perspectives, including youth’s – AYSRH health solutions can be scaled cost-effectively, at great impact and high speed.
But as we’ll also share, A360 is still learning.
We’re still striving to solve for continuation; still addressing how to resolve providers’ ingrained biases; still exploring how we can account for resource limitations all while meaningfully engaging young people throughout A360’s lifespan; and we’re still working in partnership with governments to prime interventions for the transition to health system ownership.
This ICFP, we’re reflecting: in our mission to drive AYSRH breakthrough, have we done enough as we strive to crack the code on the hardest issues facing our field?
Cracking the Code, Together
These are the top 4 questions A360 will be leaning into this ICFP:
1. How might we solve for continuation?
What A360 will be solving for: By applying our adolescent developmental science, anthropological, HCD and AYSRH lenses to understand young people’s insights, we’ve developed precise messaging that reaches young people where they are in their cognitive, social and emotional development. As a result, one in two girls who engages with A360 takes up contraception, one in two of which are long-acting reversible contraceptives (LARC). But we want to keep the long view front of mind ensuring girls who adopt methods have the support they need to continue into the future.
Where we’re headed: To help ensure girls have continuous access to the information and support they need to continue (including method switching), we’re turning to digital solutions. Through Connecting with Sara (CwS)—PSI’s technology tool to track consumers’ pathways to care—we can engage girls from referral to redemption, and beyond. In doing so, we can flag when girls report issues, like side effects, that may prompt discontinuation, and connect girls to the trusted providers to get the care they need. We launched CwS in Tanzania in August 2018. We’re monitoring the findings as we gauge how the solution can support contraceptive continuation into the future

2. How might we realistically engage young people beyond the project design?
How far we’ve come: Our mantra is clear: nothing for girls without girls. It’s not new to our project, nor this field. Integrating youth voices into A360’s transdisciplinary approach has been integral to designing youth-powered solutions. From engaging young people as designers to hiring them as staffers in implementation, we’ve been able to drill down for greater clarity on our own practices of youth engagement in each of our country contexts. But as we navigate the realities of resource constraints (human time, as well as cost), how can we best continue to prioritize meaningful youth engagement beyond the project’s lifecycle?
Where A360 is headed: As we move toward transition to government-owned implementation at scale, we’re considering: how will we keep meaningfully and realistically engaging youth so that they continue to have a seat and voice at the table, and in their health systems?

3. How might we sustain provider behavior change?
How far we’ve come: In Nigeria, preliminary findings indicate that providers who connect with girls on topics broader than contraception develop an intrinsic motivation to support girls as not just clients, but people. Despite this finding, we’re seeing that many providers still manifest a disconnect between their newfound desire to serve girls, and their ability to consistently ensure provision of a comprehensive method basket. How can we dissolve this barrier between motivation and actual execution — and how do we ensure it sticks past the period in which we’re observing providers’ interactions?
Where A360 is headed: Right now, girls are engaging with us as mystery clients to generate important data on how providers engage with girls. The insights we generate together with girls will lay our groundwork so we, as a team, can continue to explore how and where to adjust our preparation and support to providers to maintain youth-friendly services.
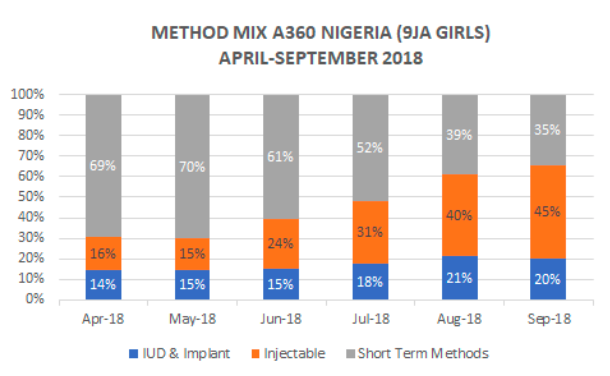
To strengthen method mix and address providers’ ingrained biases, A360’s 9ja Girls integrated the “Choice Book Method” into contraceptive counselling. The approach leads with what matters to girls, including the most effective methods for girl’s needs, the possibility for side effects and reassurance for return to fertility. Since incorporation in June 2018, 9ja Girls has recorded increased uptake of LARCs and injectable, from 15 percent in June 2018 to 20 percent in September 2018 (figure 2).
Figure 2
 4. How might we protect A360’s integrity as we transition to health system ownership?
4. How might we protect A360’s integrity as we transition to health system ownership?
How far we’ve come: Long-term sustainability lies in health system-owned implementation of these interventions. Today, we are working in close partnership with governments to ensure A360 interventions are optimally in service of government goals for adolescent health. In that process, we are exploring how best to support community structures to own demand generation, while supporting the capacity of health system actors to deliver the interventions, maintaining what makes them most effective.
Where A360 is headed: In Ethiopia, Health Extension Workers (HEWs) deliver Smart Start to rural married couples, gaining a critical asset to situate contraceptive use as relevant to girls’ immediate needs, and in service of their self-identified life goals through financial planning. The intervention has proven catalytic for HEWs: not only are couples adopting methods, but the messages are resonating with communities as a whole, and triggering shifts in health seeking behavior. As work with the Health Extension Program on Smart Start’s second iteration, we are identifying and responding to the continuing workload challenges facing HEWs. As we scale toward government integration, we’re adapting so that we support community structures to generate demand and own their health, sharing in delivery of the adolescent health package and easing the lift for HEWs, so that they can focus on sustained service delivery and follow up.

Looking Ahead
At each stage — and with each question — we’re ensuring that A360 responds to the contextual needs across the diversity of the spaces we operate. We’re continually refining and adapting so we can leave behind solutions embraced not just by the girls we serve but by the communities and health systems that will ultimately own the programs.
This journey isn’t ours alone. We’re turning to peers as we deepen our learnings, and collectively striving toward refinement of lasting, cost-efficient and resonant AYSRH breakthroughs.
I am proud of how far we’ve come, and I am energized by the opportunities ahead. This is a girl-defined revolution. We’re thrilled you’re at the forefront, learning and evolving as we go.





{kind=link}